
Have you felt a sharp pain at the tip of your shoulder? Especially when lifting overhead or during a specific portion of the bench press, have you noticed that sharp pain holding you back from expressing your strength? You've probably been diagnosed with shoulder impingement: a vague diagnosis that leaves you with the general advice of "Does that hurt? Don't do that". In the world of lifting, let me tell you: THERE IS A BETTER WAY.
We'll go into an in-depth look as to what shoulder impingement is (and more importantly, what it isn't), how it presents in powerlifting, and different ways to address it. You can also read our free guide to healthy barbell training here.
First, let's talk about what shoulder impingement is. You may hear this diagnosis under a bunch of different names like impingement syndrome, swimmer's shoulder, subacromial impingement syndrome, external impingement, and many more. Despite the various names it can fall under, shoulder impingement can be defined as "all non-traumatic, usually unilateral, shoulder problems that cause pain, localized around the acromion, often worsening during or subsequent to lifting the arm"[1]. Basically, we're discussing pain at the tip of the shoulder that is most noticeable during or after lifting your arm. For powerlifters, we tend to notice this when we're bench pressing or doing overhead press work.
Now the question is, what causes this?
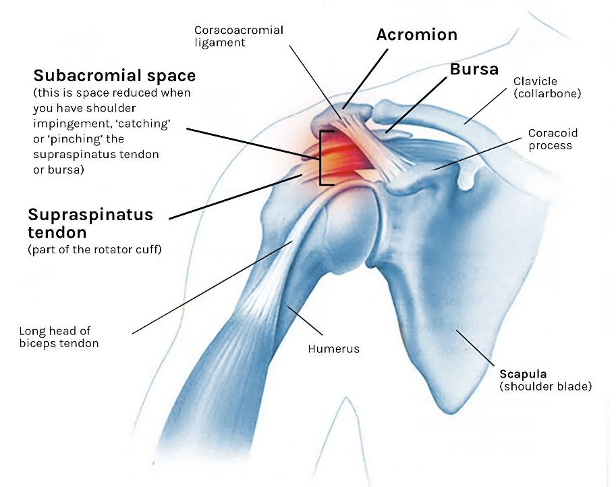
Traditionally, the term shoulder impingement was first used in 1983 but was discussed as early as 1972[2]. A doctor named Charles S. Neer argued that the shoulder structures, specifically the ones located in the subacromial space (between the acromion of the scapula and the head of the humerus) shown below, were being pinched during lifting movements, especially overhead. Whether it's the structures in the subacromial space, the actual distance between the acromion and the humeral head that makes up that space, or anything in between, damage to the structures was the primary blame for this condition. With this being the case, surgery was the recommended option of treatment. It made sense at the time; if structures seem to be the issue, changing them will address the problem, right?
Not so fast! Fast forward to today, and you’ll see, THIS IS NOT THE CASE!
We have plenty of evidence to suggest that we might have been focusing on the wrong tree in this giant forest of shoulder pain. We must understand the quality of the evidence that the theory of shoulder impingement was founded. The report in 1972 that discussed shoulder impingement and the surgery to address it was not a robust scientific paper at all. According to an editorial by Jeremy Lewis, by today's standards, this report would meet the quality of a blog [2]. Nowadays, we look to the totality of the evidence in scientific literature to guide our approach. With that, it's time for an update.
Let's discuss why it's so important that we need to understand that structure is not the only factor with shoulder impingement.
Imagine this: You get frustrated with your shoulder pain since it keeps bothering you every time you bench press.
You begin to dread each session, knowing the outcome will be the same. So, you decide to go to the doctor. They twist, bend, and crank on your shoulder for a whopping 3 minutes, leading to them saying, "You have shoulder impingement, don't lift for a couple of weeks. If it stays the same or gets worse, we'll look into surgery". You follow up with a question, "Is surgery really necessary?" Only to receive a less than sufficient reply. You'll probably hear, "Well, if it keeps hurting, it means the bones are rubbing against the tendons and other structures in the shoulder, which can lead to wear and tear damage. We need to go in and address that rubbing". That kind of makes sense, right? If this bony "impingement" on the soft tissues in my shoulder is the cause of my pain, fixing that will get rid of the pain… supposedly.
However, with the recent evidence science has revealed, we know that the answer is not this simple!
Many studies investigate what contributes to shoulder impingement as well as what treatments are effective for it. As I have mentioned before, we can't solely blame the tissues rubbing against the bone for this pain we're experiencing. A great example of this can be seen in evidence that relates to surgery vs. conservative treatment. Participants who underwent the actual surgery to address shoulder impingement compared to participants who received a placebo arthroscopy (the surgeons went in but made no structural changes) showed no differences in pain severity when reassessed for up to 24 months[3]!
That’s huge!
This is one of many articles of evidence that show, in the absence of trauma, we can still get better even if we don't change the structures in the shoulder. To add on to that, remember when we briefly mentioned there are those who blame the actual distance in the subacromial space as a driver of pain? Well, that has been debunked [4]. Long story short, surgery is NOT the best answer… so what is?
MOVEMENT!
Now why is this the case? Well, to explain the findings of the previously mentioned studies[3,4], think about it this way: Your bones have always been that way! Whether the acromion is more hooked or there is less distance in your subacromial space, chances are your shoulder has had those characteristics for a long time throughout your development as a human. So, it’s not so much the structure causing the issue as much as it is other potential factors that relate to our training. We want to TREAT THE ISSUES, NOT THE TISSUES. These issues include, but are not limited to, sudden changes in volume or intensity that we are not adapted to, life stressors, a change in our movement mechanics, and more. If you want to read more about this, check out Dr. Rori Alter’s article entitled “Treat the issues not the tissues”.
There is a growing body of evidence to support exercise as the first-line defense against shoulder impingement[5]. Whether it's regular exercise or even movements on the Wii gaming system[6], we need to find a way to modify our training variables and move to calm things down so we can build them back up.
Now that we understand what shoulder "impingement" is and is not, let's talk about how it relates to powerlifting and look at practical steps you can take if you're dealing with this issue.
There is a massive benefit of using exercise to rehab, especially if you train with the main powerlifting movements. Long story short, we can modify the movements you train with as rehab.
Meaning, we can still do what we love to do while staying on track towards our goals. There are general steps to take with regards to modifying training to address this pain.

But first, we need to take a look at how this all started. Was there an acute trauma that caused immediate pain? Or was it a little pain that built up over time and has become unbearable? These questions are essential because they can shape how we approach our pain. If the pain resulted from acute trauma, reach out to a healthcare professional that can assess you, and figure out the best course of action for you. If it was a pain that built up over time, the next couple of steps could help a ton.
After looking at our situation, we need to figure out what makes the pain better or worse. The most straightforward starting point we can address is either weight on the bar or technique. Can you take some weight off the bar that allows you to train the intended movement? Or do you notice the pain even with the empty bar? Can you modify your grip or chest position on the bench press? Or is the pain there no matter what technique change you make? If weight change or technique change allows you to train without aggravating your pain, start there.
If changing the weight on the bar does not help, we can look at the range of motion you are performing. Does a certain point in the range of motion cause shoulder pain during the bench press? Shorten it! For example, if you experience shoulder pain when the bar reaches your chest, you can hover just above that point.
One thing to keep in mind is that powerlifting is a sport. With that sport comes rules. The bar must remain still on the chest with the bench press before you push the bar off to lockout. In the previous example, we recommended hovering over the chest. However, this does violate one of the rules of the lift. With that being said, we cannot avoid this position forever. What do we do in the meantime? We can find a variation that allows us to train the aspects of the sport we need to while letting the pain calm down. It's the best of both worlds! So, as things start to calm down, we continue to progress towards the original competition lift while respecting the progress being made. Using an exercise variation can also be a significant step to consider if modifying the range of motion doesn't help.
One last point to consider is often not addressed nearly as often as it should: psychosocial factors.
Your approach with this needs to be based on factors that relate to your concerns, beliefs, and what is important to you! Ask yourself: What are your expectations of this experience? Are you expecting a complete recovery overnight or slight improvements over time? Do you feel that you can manage this on your own? Or do you feel like this is entirely out of your control? These questions are important because they can determine how we cope with pain if our expectations are realistic, given the presentation and our confidence in our ability to manage this on our own. The goal is to move towards an approach that puts you in the driver's seat. These expectations and improved self-efficacy can lead to better outcomes[7,8].
If you would like some practical analogies to help navigate shoulder pain, I wrote an article entitled “3 Analogies to Help You Barbell Train Even When You’re in Pain!”.
As we come to a close, here are some key points to remember:
Shoulder impingement is a biomechanical observation more than it is a diagnosis.
You can get better without changing the tissues surgically with conservative treatment.
You can modify your powerlifting training as a rehab tool rather than avoid it as most practitioners would recommend
Don't ignore the significance of psychosocial factors. Addressing the way you cope with this experience can be a key player in your return to powerlifting.
At the end of it all, shoulder impingement is not a fun "diagnosis" to receive. This shoulder pain can be a frustrating experience and, coming from a recreational powerlifter who has dealt with bilateral shoulder pain that presents like this, I can relate.
If you are experiencing severe, overwhelming pain that disrupts your life, pain is getting worse, or all of the above: seek help from a clinical professional who will guide you through the process and keep you doing what you love!
Dealing with chronic or acute injuries interrupting your training? Book a free call with a PRS Clinical Coach today to get some answers!
If you're interested in learning how to optimize barbell technique, maximize strength and muscular development, and reduce injury risk (and peeing) for you, your clients or patients, then join the waitlist to get insider information on all the PRS online courses when they're ready for enrollment!
REFERENCES:
Diercks R, Bron C, Dorrestijn O, et al. Guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review by the Dutch Orthopaedic Association. Acta Orthop. 2014;85(3):314-322. doi:10.3109/17453674.2014.920991
Lewis J. The End of an Era?. J Orthop Sports Phys Ther. 2018;48(3):127-129. doi:10.2519/jospt.2018.0102
Paavola M, Malmivaara A, Taimela S, et al. Subacromial decompression versus diagnostic arthroscopy for shoulder impingement: randomised, placebo surgery controlled clinical trial. BMJ. 2018;362:k2860. Published 2018 Jul 19. doi:10.1136/bmj.k2860
Park SW, Chen YT, Thompson L, et al. No relationship between the acromiohumeral distance and pain in adults with subacromial pain syndrome: a systematic review and meta-analysis. Sci Rep. 2020;10(1):20611. Published 2020 Nov 26. doi:10.1038/s41598-020-76704-z
Pieters L, Lewis J, Kuppens K, et al. An Update of Systematic Reviews Examining the Effectiveness of Conservative Physical Therapy Interventions for Subacromial Shoulder Pain. J Orthop Sports Phys Ther. 2020;50(3):131-141. doi:10.2519/jospt.2020.8498
Rizzo JR, Thai P, Li EJ, et al. Structured Wii protocol for rehabilitation of shoulder impingement syndrome: A pilot study. Ann Phys Rehabil Med. 2017;60(6):363-370. doi:10.1016/j.rehab.2016.10.004
Chester R, Jerosch-Herold C, Lewis J, Shepstone L. Psychological factors are associated with the outcome of physiotherapy for people with shoulder pain: a multicentre longitudinal cohort study. Br J Sports Med. 2018;52(4):269-275. doi:10.1136/bjsports-2016-096084
Meehan K, Wassinger C, Roy JS, Sole G. Seven Key Themes in Physical Therapy Advice for Patients Living With Subacromial Shoulder Pain: A Scoping Review. J Orthop Sports Phys Ther. 2020;50(6):285-a12. doi:10.2519/jospt.2020.9152